Unprescribed: Legislation to Keep Drugs Out of Water Thwarted by U.S. Pharmaceutical Lobbying
An estimated 10 to 40 percent of prescription and over-the-counter medicines are not used, but how to properly dispose of these drugs depends on who you ask. Since there is no continuous national program, states — and even some cites — are instituting their own regulations, but not without complaints from the pharmaceutical industry.

By Brett Walton
Circle of Blue
At least a decade after analytic technology became sensitive enough to detect pharmaceuticals at concentrations of parts per trillion — or one drop in a thousand Olympic-sized swimming pools — nearly half of the states in the union have proposed legislation to encourage safe disposal of prescription medications. Because trace levels of pharmaceuticals have been detected in drinking water and linked to abnormalities in aquatic organisms, drug-disposal legislation has attracted broad support from public health officials, law enforcement agencies, and environmental groups.
Yet the U.S. pharmaceutical industry, whose twelve largest companies made a profit of $US 44 billion in 2010, have countered with a coast-to-coast campaign to prevent lawmakers from making the industry pay for drug-disposal programs, asserting that the programs have little effect on water quality, are burdensome to the consumer, and could lead to drug theft and abuse.
— Margaret Shield
Hazardous Waste Liaison
King County, Washington
The debate over the relevance of these programs, which would involve new state safety regulations, pits expanding knowledge about the risks of minute concentrations of prescription drugs in the nation’s waters against a powerful industry’s resistance to governmental safety mandates. The contest comes during an era of economic distress in the United States that has prompted fresh doubts among many citizens about the effects of health and environmental regulations on the nation’s economic performance. Health and environmental advocates, meanwhile, contend that fouling the nation’s waters with prescription drugs and prompting higher levels of human disease represents a much larger threat to the economy and the nation’s well-being.
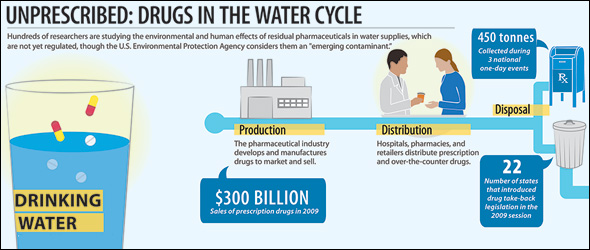
In 2009, some 3.9 billion prescriptions — topping $US 300 billion in sales for the first time — were dispensed in the U.S., according to IMS Health, a market research company. Sales nearly doubled over the last decade, and the baby boomers, all 78 million of them, are reaching the age when prescription drug use increases.
There is a wide range of estimates for how many of those drugs go unused. The pharmaceutical industry maintains that the figure is 10 percent. According to research from the Unused and Expired Medications Registry, which keeps a large database on such matters, an estimated 40 percent of medications are not taken by the consumer and need to be disposed.
State Programs: Popular, Successful, and Broke
In September U.S. Representative Louise Slaughter, a New York Democrat, introduced legislation that would create a national industry-funded drug take-back program. Since no such permanent program now exists, some states are responding with their own plans, which are quickly running out of money. Cities and counties also run small-scale collection programs, using drop boxes or collaborations with pharmacies.
“The question is: who is going to pay?” Margaret Shield told Circle of Blue. Shield is the policy liaison for the Local Hazardous Waste Program in King County, Washington. “The drug industry can incorporate a program into the cost of business, and they’re saying no.”
Maine’s landmark program — the first statewide program in the nation when it began in 2007 — will exhaust its funding by the end of the year.
“Our state, like many, is broke,” Jennifer Crittenden, Maine’s program director since its inception, told Circle of Blue. “We’ve had a change in government administration with different priorities. There are no plans to continue funding the program.”
Crittenden said Maine’s program has been “immensely successful” and that it became a national model. The total annual cost for the program, which collected just over one metric ton (2,373 pounds) of drugs in its two-year pilot phase, is $US 75,000.
Because of budget austerity, five states — Florida, Maine, Minnesota, Oregon, and Washington — submitted bills during the 2009-10 legislative session that would have required the pharmaceutical industry to pay for drug disposal: none of these bills passed. The only industry-funded program is at the city level, in San Francisco.
Likewise, Iowa, Nebraska, and New Hampshire have enacted statewide drug take-back programs, which allow customers to drop unwanted pills at the pharmacy or to mail leftover medicines to a collection center, and 20 other states have introduced similar legislation to set up full-time programs or trial studies.
Kate Gainer, who administers the take-back program in Iowa, said she has had a different funding partner each year since the program started in 2009. “We’ve tried different angles but haven’t identified a sustainable source,” Gainer told Circle of Blue. “We pursued pharmaceutical avenues, but that was not successful.” The Iowa program has received nearly 10 metric tons (21,545 pounds) of returned drugs in just two years.
In Colorado, the same dynamic holds: Greg Fabisiak, who manages the state’s pilot project for the Department of Public Health and Environment, said the main challenges were finding funding and operating a large-scale program. The pilot project has only 11 drop-off locations in the entire state, but has collected 5.5 metric tons (12,000 pounds) of drugs since 2009.
New Protections Merited
Certainly, say advocates of drug-disposal legislation, the scientific evidence merits new safeguards. Numerous studies have observed fish developing sexual and behavioral abnormalities, such as males producing eggs or females disinclined to spawn. The scientific consensus is that pharmaceuticals threaten aquatic organisms, though the effects on human health are not as clear.
Pharmaceutical chemicals and hormones have reportedly been detected in the drinking water for at least 14 percent of Americans, according to test results from utilities and independent researchers published by the Associated Press in March 2008. Most worrisome are the endocrine disruptors — a sub-class that includes the estrogen used in birth control and bisphenol A used in plastics — which interfere with hormones and can lead to abnormal sexual development in fish, frogs, and even humans.

More than a year and a half later, in October 2009, the Obama administration released an updated guideline for how to safely dispose of the millions of pounds of medications that expire or go unused in the United States each year. Further, there have been three national take-back events since September 2010, with the most recent last Saturday, October 29, though there is currently no continuous national drug-disposal program.
Instituting take-back programs will be easier, now that the U.S. Congress passed a bill last year allowing changes to the Controlled Substances Act. Currently, controlled substances — such as narcotics and Oxycontin — can be handled only by law enforcement officers, meaning those pills cannot be returned to pharmacies. The U.S. Attorney General is expected to announce the specific policy changes this fall.
However, efforts to establish a sustainable source of funding to change ideas about drug-company responsibilities have failed so far, largely because of strong opposition and lobbying from the pharmaceutical industry, which does not want industry-funded programs to become a legal precedent. The bill in Washington state, for example, would have cost pharmaceutical manufacturers 1.5 cents per prescription.
Big Industry Lobbying Big Dollars
As late as 2007, the U.S. government encouraged people to dispose of certain medications by doing what health and environmental advocates now discourage — flushing them down the toilet so that they would not result in accidental poisoning, theft, or prescription drug abuse.
Since the mid-1990s, however, drug take-back programs have cropped up around the world as part of a wider “product stewardship.” An industry-funded model is standard in Australia, as well as in many European countries and Canadian provinces.
Though industry lobbying has successfully blocked all state attempts for such programs in the U.S., the nation’s first industry-pays model began this fall in San Francisco at the city level. The one-year pilot program carries a price tag of $US 110,000, with more than 90 percent being covered by Pharmaceutical Research and Manufacturers of America (PhRMA), the lobby group for drug research and biotech companies, and the remainder handled by Genentech, a biotechnology company.
The San Francisco Board of Supervisors passed a bill through committee for an industry-funded program, but the bill never came up for a full vote because industry representatives wanted to negotiate the outcome, said Caitlin Sanders, a toxic substances specialist at the San Francisco Department of the Environment
Shushma Bhatia, the toxics reduction program manager for the department, told Circle of Blue that the regulations for the program have been written, but the city still needs to find a vendor to manage collection and disposal.
These local and state programs have proved popular, and single-day national collection events, coordinated by the U.S. Drug Enforcement Agency (DEA), have exceeded expectations. During the three Saturday events in the last 13 months, law enforcement agencies throughout the country set up temporary collection sites, where citizens, sometimes toting pill-filled kitchen-drawers, have deposited nearly 450 metric tons (1 million pounds) of unwanted medications.

“The amount of prescription drugs turned in by the American public during the past three Take-Back Day events speaks volumes about the need to develop a convenient way to rid homes of unwanted or expired prescription drugs,” said DEA Administrator Michele M. Leonhart, in a press statement. “DEA remains hard at work to establish just such a drug disposal process, and will continue to offer take-back opportunities until the proper regulations are in place.”
But if those regulations would make drug companies pay, the industry wants no part of it.
During the 2009-10 legislation session in Maine — which was considering industry-pays legislation — there were advertisements in state newspapers claiming that take-back programs would increase the cost of health care, would not have a positive effect on water quality, and would create an opportunity for theft. These ads were paid for by the Generic Pharmaceutical Association (GPhA), the lobby group for generic drugs, and PhRMA, which has, since 1998, ranked fifth in the nation for lobbying expenditures, spending $US 90.7 million on lobbying activities in the U.S. from 2007 to 2010, according to the Center for Responsive Politics.
In a January 2011 comment to a report on product stewardship by Maine’s Department of Environmental Protection, the GPhA praised Maine’s legislature, which “wisely rejected” a pharmaceutical take-back program that was projected to cost $US 1.5 million annually for three years, “after which the annual cost would be unlimited.” The GPhA criticized the mail-back component of the program, stating that the estimated costs were $US 7.50 to $US 17.00 per envelope, since some generic medicines only cost $US 4 for a 1-month supply. The GPhA went on to say that effective and affordable take-back programs could be instated, “without mandating manufacturer-funded programs that risk increasing health care costs.”

Additionally, the comment mentions Raanan Bloom, the FDA’s environmental assessment expert, who says “the main way drug residues enter water systems is by people taking medications and then naturally passing them through their bodies.” According to the GPhA, it is estimated that more than 90 percent of the trace medicines found in surface water is excreted, rather than discarded or flushed:
“Thus, even if a costly program were 100 percent effective, it would do little if anything to impact the amount of pharmaceuticals entering water systems. In addition, experts agree that there is no scientific evidence to demonstrate that the traces of pharmaceuticals detected in water have any impact to humans.”
Widespread, But Miniscule
Pharmaceutical take-back programs are a multi-faceted issue. Advocates for take-back programs acknowledge that improper disposal is a small source of environmental contamination, compared to amounts that are excreted in bodily waste. They also recognize that the concentrations in rivers and lakes are millions of times smaller than prescribed doses, meaning the threat to human health is minimal, though consensus is that the same cannot be said for aquatic life.
Since the 1970s, the academic community has been aware of minute concentrations of pharmaceuticals in drinking water. But because the concentrations are so low — usually measured in parts per trillion, or thousands of times smaller than prescribed doses— it is only recently that monitoring technology has become sophisticated enough for detection.
About a decade ago, environmental advocates became concerned after the U.S. Geological Survey (USGS) completed the first national evaluation, sampling water in 30 states. Published in 2002, that study found detectable levels of pharmaceuticals in 80 percent of the 139 streams tested.
Then, in March 2008, the Associated Press brought public attention to the issue with its investigative series that revealed traces of pharmaceuticals in the drinking water of 41 million Americans in 24 major metropolitan areas. The AP’s findings led to hearings at the local, state, and federal levels. At a committee hearing in April 2008, Senate Democrats rebuked the Environmental Protection Agency (EPA) for not doing its job.
Since the 2002 USGS study, hundreds of tests have been carried out on water bodies across the U.S. The EPA maintains a database with thousands of research papers on the environmental contamination caused by pharmaceuticals and personal care products, or PPCPs. This is a broad designation for a class of more than 1,500 FDA-approved substances used in everything from Advil and antidepressants to soaps, lotions, and veterinary medicines — basically, anything humans or their pets put on their bodies that is not clothing and anything ingested that isn’t food.
Potential Threat: Fish Only?
Of the more than 1,500 identified compounds, only a couple dozen have ever shown up in treated drinking water that is supplied to homes. Fear of the human defects, however, is based more on assumption than empirical evidence. Scientists have not found a direct effect on humans from long-term, chronic exposure to PPCPs, mostly because it is too early in the research cycle for those studies to have been completed. A World Health Organization summary report released in June concluded that, though available data is limited, there is a “substantial margin of safety” between the concentrations currently in drinking water and the concentrations that would be needed to cause harm to humans.
Though human health is an assumed but unsubstantiated concern, the greatest immediate risk is to aquatic organisms, which have constant, prolonged exposure to contaminated water. These effects can move up the food chain, compounding at every trophic level, from the smallest organisms to the largest, with pharmaceuticals turning up in fish tissue. Furthermore, there is scientific evidence that these contaminants have altered the reproductive behavior and sex ratios of several species of fish.
Additionally, pharmaceutical-laden water is an ideal petri dish for nurturing that perpetual public health nightmare — antibiotic-resistant bacteria. Continuous exposure to low doses of medications would allow water-borne microbes to build immunity to the drugs that are designed to kill them.
Other Solutions
Despite this, the EPA does not regulate PPCPs, and most wastewater treatment facilities are not equipped to remove all of them. Doing so would require revamping the treatment process.
“We’re talking reverse osmosis and membrane technology everywhere, and that gets expensive,” said Gabriel Eckstein, a law professor at Texas Wesleyan University who has co-authored a report on keeping pharmaceuticals out of water bodies without relying on regulatory bulwarks like the Clean Water Act and the Safe Drinking Water Act.
Take-back programs are just one relatively inexpensive process that can be used to prevent unused medications from entering water supplies, according to Sierra Fletcher of the Product Stewardship Institute, an advocacy group. The more fraught aspects — such as drugs designed to be fully metabolized and upgrades to wastewater treatment plants — will be significantly more expensive and will require years for development.
“We don’t have a product-stewardship culture in the U.S.,” California State Senator Joe Simitian, a Democrat, told Circle of Blue. Simitian sponsored a bill — which passed in 2007 — to create guidelines for take-back programs in the state, but he doesn’t see the same vigor at the state or national level as in San Francisco.
“It’s difficult,” Simitian said, “because it’s a significant change in mindset. We’re trying to reshape the way we think about things in what is currently a throw-away world. It’s easier if there’s one obvious responsible party. But is it who makes the drug? Who sells it? Who buys it? Once that begins, everyone agrees there is a problem and something should be done, but somebody else should do it.”
Brett Walton is a Seattle-based reporter for Circle of Blue. Contact Brett Walton

Brett writes about agriculture, energy, infrastructure, and the politics and economics of water in the United States. He also writes the Federal Water Tap, Circle of Blue’s weekly digest of U.S. government water news. He is the winner of two Society of Environmental Journalists reporting awards, one of the top honors in American environmental journalism: first place for explanatory reporting for a series on septic system pollution in the United States(2016) and third place for beat reporting in a small market (2014). He received the Sierra Club’s Distinguished Service Award in 2018. Brett lives in Seattle, where he hikes the mountains and bakes pies. Contact Brett Walton








The Yellow Jug Old Drugs program has 215 participating pharmacies across Michigan. The Program is funded by community-minded pharmacies and program sponsors. In two years time, the program has collected over 26,000 lbs to date.
The program will be expanding to other Great Lakes states in 2012.
Chris Angel, President
Volunteer Board of Directors
Great Lakes Clean Water Org
http://www.greatlakescleanwater.org
Proper disposal of pharmaceuticals should NOT be the problem of the drug companies. If we did have a secure method of disposal that would not further harm the environment, we should consider it, but how do we separate out the active metabolites of all the $400 billion worth of prescriptions consumed in the country? Water treatment plants to ramp up treatments to remove organics etc.? Can we afford water at 5-10 times the current municipal price? I don’t think so.
Legislation may not be required, educating the consumer as to the health effects could just as helpful. It will take time, but if you add labeling, PSAs and teach conservation at the local schools it will start to naturally decline. It won’t fix the problem but could help. Just a thought.